Ovarian Cysts
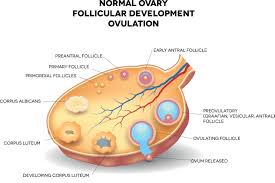
Ovarian cysts are fluid filled sacs that form on the ovary. These cysts are very common and occur every month when your ovary is stimulated by your brain to release an “egg” during ovulation. We use the term cyst and follicle interchangeably and sometimes this can be very confusing for patients.
What can cause an ovarian cyst?
- Ovulation: If you are not in menopause, every month one of your follicles is stimulated to mature. As the follicle grows it forms a little cyst which will eventually rupture mid-cycle releasing the egg. These are called “functional” ovarian cysts and they do not need surgical intervention as they typically resolve on their own.
- Dermoid cyst: Are made of “germ cells” which are present since you were a fetus growing in your mother’s belly. They are also called teratomas and can contain teeth, hair, nerve cells, fat…pretty much any type of tissue found in your body. They are usually found in women once a doctor does an ultrasound which is usually between the ages of 20-40. These types of cysts are usually benign but once found should be removed because a rare form of teratoma can be cancerous.

Teratoma with teeth 
Teratoma with a tooth and hair

3. Polycystic Ovarian Syndrome (PCOS): Women with PCOS have difficulty with ovulation and if you do not ovulate, the follicles never rupture which means that the ovary is left with many small cysts that over time can become very large and painful. Birth control pills can help 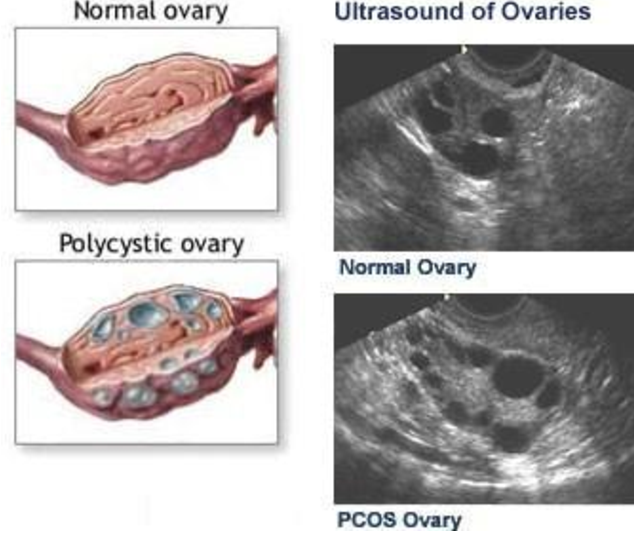
4. Endometriosis: Women with endometriosis can form “endometriomas” which are ovarian cysts filled with blood. When the blood is trapped and kept in place for a while, it darkens. During surgery, if the endometrioma is ruptured, the blood looks like dark chocolate so another name for endometrioma is “chocolate cyst”.
5. Pregnancy: Believe it or not, pregnancy has a cyst that supports the pregnancy during the first twelve weeks of gestation until the placenta develops. This cyst is called a corpus luteum cyst and it is completely benign. It usually resolved on its own by week 12 of gestation.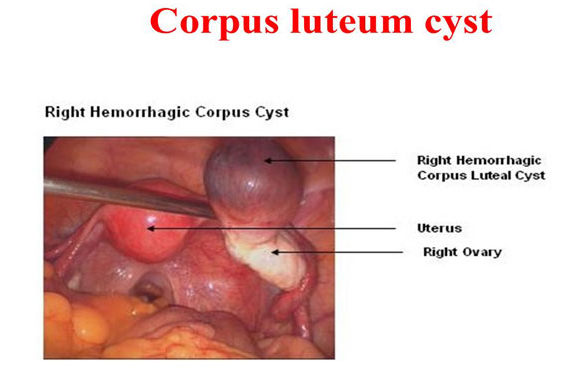
6. Infections: If you get pelvic inflammatory disease from either a sexually transmitted infection or a ruptured appendix, your body will form a cyst wall around the infection called an abscess. These are cysts that are filled with pus. They can either be drained through the vagina with the help of interventional radiology or surgically. These types of infections require antibiotics to prevent spread and fertility issues.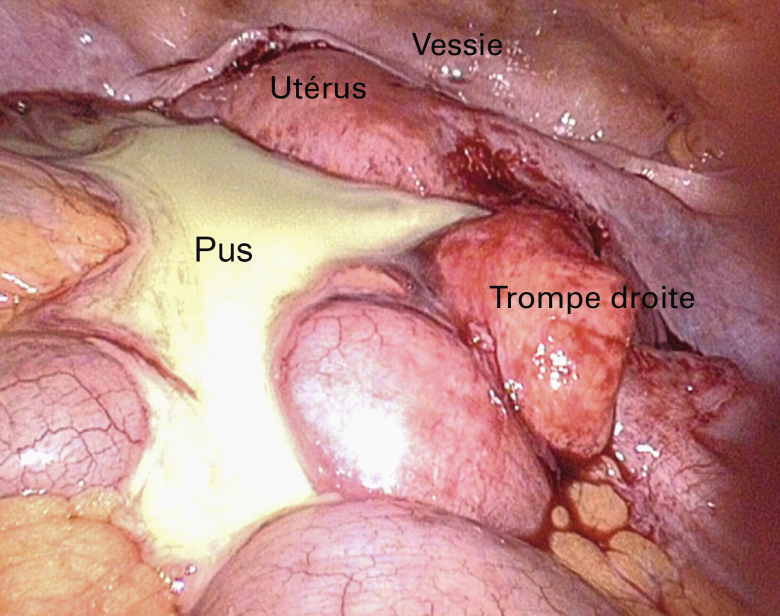
7. Cancer: less than 1% of ovarian cysts are cancerous
What are my risks of ovarian cancer if I have a cyst?
Ovarian cancers are extremely rare but there are certain women who may have a higher risk:
- Family history or genetic predisposition
- Previous history of breast or intestinal cancer
- A cyst that appears complex & suspicious with solid and multiple fluid filled areas
- Fluid collection outside the cyst wall. Fluid in the abdominal cavity called ascites
What are some symptoms I may feel if I have an ovarian cyst?
- Cramping abdominal pain or pressure, dull ache may be constant or intermittent
- If the cyst ruptures, the pain can be sharp and excrutiating
- If the cyst twists in on itself (torsion) you can get nausea and vomiting, this requires surgery to save the ovary because torsion can cut off the blood supply to the ovary
How do we diagnose an ovarian cyst?
- Pelvic exam this is why your annual exams are so important
- Ultrasound
- CT or MRI
What can a blood test tell me about my cyst?
- Pregnancy test: will let you know if the cyst might be a corpus luteum cyst
- CA-125: can be elevated in endometriosis and cancer. Should only be ordered if a cyst appears suspicious or in a post menopausal female
- HE-4: produced by epithelial ovarian cancer cells. Can help you differentiate between and endometrioma and an ovarian cancer. HE4 will be low in patients with endometriosis
Treatment:
- Watchful waiting: if no symptoms and the cyst does not appear suspicious, you can repeat the ultrasound in 6 wks to see if it will stay the same, resolve or grow
- If tumor markers are elevated: surgery to remove the cyst or the ovary
- If the cyst is greater than 5cm: more likely to require surgery because of the risk of ovarian torsion.